Safe Exercise After Head Injury: Your 2026 Guide
June 15, 2026


Safe exercise after head injury is defined as physical activity performed below the intensity that triggers symptom worsening, a clinical approach known as sub-symptom threshold exercise. The 2023 Amsterdam Consensus Statement confirms that early sub-threshold aerobic exercise accelerates concussion recovery rather than delaying it. That finding overturns the old “complete rest until symptom-free” advice that kept many patients on the couch far too long. The key is not avoiding movement. The key is moving at the right intensity, tracking your symptoms honestly, and progressing one stage at a time.
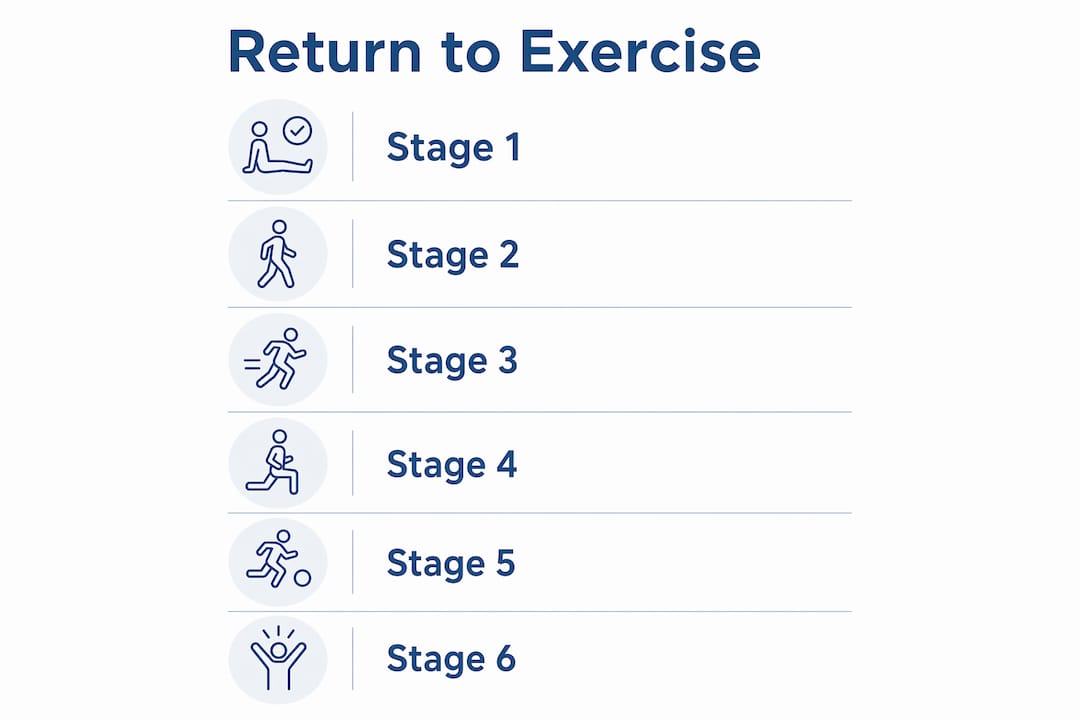
The graded 6-stage return-to-play protocol is the most widely used clinical framework for physical activity after brain injury. Each stage requires a minimum of 24 hours without symptom worsening before you advance. Rushing that timeline is the single most common mistake people make.
The stages move from the gentlest aerobic work to full contact activity. Here is how each level looks in practice:
Vestibular rehabilitation exercises are a separate but equally important category of rehabilitation exercises after concussion. These target the inner ear and gaze stability systems that often malfunction after a head injury. Gaze stability exercises, including VOR x1 drills, saccades, and habituation movements, retrain your brain to process visual and balance signals accurately.

The critical rule here is controlled exposure. You want to provoke mild dizziness, not severe spinning. If a gaze exercise makes you feel moderately unsteady for 20–30 seconds and then settles, that is therapeutic. If it triggers a headache that lasts an hour, you went too far.
Pro Tip: Start vestibular exercises seated before attempting them standing. Seated practice reduces fall risk while still challenging your balance system effectively.
One important caution: resistance training early in recovery raises both intracranial and blood pressure, which can worsen post-concussion symptoms significantly. Limit yourself to light bodyweight movements only in the first two stages, and only if they feel tolerable.
The sub-symptom threshold concept means your exercise intensity must stay below the point that causes symptom flare-ups to remain therapeutic. Exercise near the symptomatic threshold actually improves brain autoregulation, which is the brain’s ability to regulate its own blood flow. Going over that threshold does the opposite.
Rate each of your primary symptoms on a 0–10 scale before you start exercising. Common symptoms to track include:
Record your baseline score for each symptom. Check in again at the midpoint of your session and immediately after finishing.
The two-point rule is a clinical benchmark used widely in concussion therapy. Stop exercising immediately if any symptom increases by 2 or more points from your baseline score. A symptom jump of that size signals that you have crossed your threshold and risks triggering a symptom crash that can set your recovery back by hours or even days.
“Symptom exacerbation greater than 2 points causes a ‘symptom crash’ that can delay recovery for days.” — Remote Rehab Physiotherapy
Pro Tip: Wear a heart rate monitor during every session. Knowing your exact heart rate helps you stay under 55% of your maximum in early stages without guessing.
Consistent 15-minute daily sessions of light walking outperform sporadic longer workouts for brain recovery. Short, regular doses retrain your autonomic nervous system steadily. One 45-minute session every few days does not produce the same result.
Creating a safe space for home-based exercise matters as much as choosing the right activity. Vestibular exercises intentionally provoke mild dizziness, so your environment needs to account for that reality.
| Equipment | Purpose | Stage to introduce |
|---|---|---|
| Stationary bike | Low-impact aerobic exercise with no fall risk | Stage 2 |
| Heart rate monitor | Keeps intensity below symptom threshold | Stage 2 onward |
| Resistance bands | Light resistance training with low pressure | Stage 3–4 |
| Foam pad | Adds balance challenge for vestibular drills | Stage 3 onward |
| Treadmill (low speed) | Controlled walking with handrail support | Stage 2–3 |
Safety setups like the corner technique are not optional extras. They are standard clinical recommendations because vestibular exercises are designed to challenge an already impaired system.
Pro Tip: If you exercise outdoors, choose flat, familiar routes with minimal traffic noise and visual complexity. Busy intersections and uneven terrain add sensory load that can push you over your symptom threshold faster than the physical effort alone.
Most setbacks in physical activity after brain injury come from a small set of predictable errors. Recognizing them early keeps your recovery on track.
Mild symptom increases during exercise are acceptable and expected. Moderate to severe increases are not. Many people confuse discomfort with progress and push harder when symptoms spike. That approach does not build resilience after a head injury. It triggers symptom crashes that force days of rest and erase recent gains.
“Scaling back upon symptom flare avoids setbacks lasting hours or days.” — Remote Rehab Physiotherapy
Patients often attempt long, infrequent, intense sessions instead of short daily ones. A 45-minute run once a week feels more productive than a 15-minute walk every day. For concussion recovery, the opposite is true. Regular micro-doses of exercise retrain the autonomic nervous system far more effectively than occasional high-effort sessions.
Many people focus only on aerobic exercise and ignore vestibular rehabilitation. If you have ongoing dizziness, balance problems, or visual disturbances, aerobic exercise alone will not resolve those symptoms. Vestibular rehab requires its own dedicated program, ideally supervised by a trained clinician.
The most important adjustment you can make after a setback is reducing volume before reducing frequency. Keep showing up daily, but do less each session until your baseline stabilizes again.
Safe exercise after head injury requires consistent, symptom-guided progression through defined stages, not rest alone or aggressive training.
| Point | Details |
|---|---|
| Start with sub-threshold aerobic work | Keep heart rate at or below 55% of your maximum in early recovery stages. |
| Use the two-point rule every session | Stop immediately if any symptom rises 2 or more points from your pre-exercise baseline. |
| Add vestibular rehab alongside aerobics | Gaze stability and balance drills address dizziness and coordination that aerobic exercise alone cannot fix. |
| Prioritize daily short sessions | Fifteen minutes of daily light exercise outperforms sporadic longer workouts for brain recovery. |
| Set up a safe home environment | Use the corner technique, clear your floor, and keep a chair nearby during all balance exercises. |
I have worked with a lot of people who came in convinced that rest was the answer. They had been told to sit in a dark room, avoid screens, and wait. Some of them waited weeks. A few waited months. By the time they arrived, their symptoms had not resolved. In many cases, the prolonged inactivity had made things worse.
What I have found, consistently, is that the patients who recover fastest are not the ones who push hardest. They are the ones who show up every single day and do a little. Fifteen minutes of walking. A few minutes of gaze stability work. Nothing dramatic. Just steady, symptom-guided effort repeated daily.
The psychology of returning to physical activity after a head injury is genuinely difficult. You feel fragile. You are afraid of making things worse. That fear is understandable, but it becomes its own obstacle when it keeps you completely still. The research is clear that early controlled activity supports recovery. The goal is not to be fearless. The goal is to move carefully and trust the process.
I also want to be direct about the opposite error. Some patients, especially athletes, treat symptom monitoring as optional. They push through headaches and dizziness because they are used to training through discomfort. That instinct does not transfer to concussion recovery. The brain is not a muscle that gets stronger from being overloaded during injury. It needs calibrated challenge, not brute force.
Patience and consistency are not passive. They are the active ingredients in this process.
— Chad
Recovering from a head injury is not something you should navigate alone, especially when exercise intensity and symptom monitoring need to be precisely calibrated for your specific situation.
At Brainrestoremeridian, our team in Meridian, Idaho specializes in personalized concussion rehabilitation, including supervised sub-symptom threshold exercise programs, vestibular rehab, neurofeedback, and hyperbaric oxygen therapy. We build individualized recovery plans that account for where you are right now and where you need to go. Whether you are in the earliest stages of recovery or stuck at a plateau, we can help you move forward safely and confidently. Reach out to Brainrestoremeridian today to schedule your consultation and take the first real step toward reclaiming your physical independence.
You can begin light aerobic activity, such as walking or stationary cycling, as soon as your symptoms are manageable and you can stay below your symptom threshold. The 2023 Amsterdam Consensus Statement supports early sub-threshold exercise as beneficial for recovery.
Short walks and gentle stationary cycling at no more than 55% of your maximum heart rate are the safest starting points. Avoid resistance training, high-impact activities, and any exercise that raises intracranial pressure in early recovery.
Use a 0–10 symptom scale before and during exercise. If any symptom increases by 2 or more points, stop immediately. That two-point rule is a standard clinical benchmark for preventing symptom crashes during concussion rehab.
The graded 6-stage return-to-play protocol requires at least 24 hours of symptom-free progression at each stage, so the minimum timeline is several days. Most people take weeks to months depending on injury severity and consistency of their rehab program.
Professional supervision is strongly recommended, particularly for vestibular rehabilitation exercises and for anyone whose symptoms are not improving. A trained clinician can prescribe the correct exercise intensity, monitor your response, and adjust your plan when setbacks occur.

